Before class
1. Human health and the environment
3.1 learning outcome:
Understand the link between planetary health and human health
Concept check:
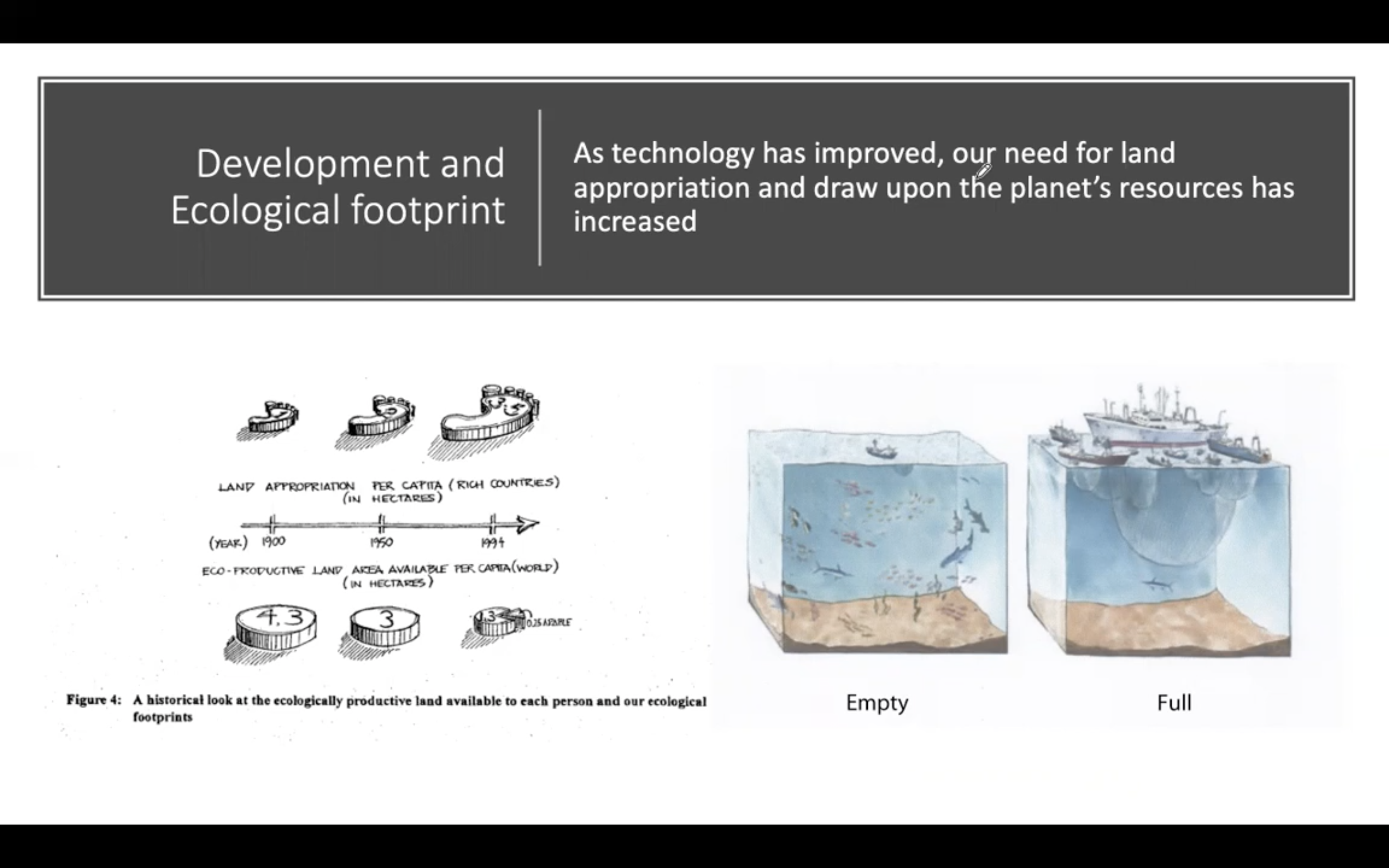
Ecological foot print
: The load imposed by a given population on nature
> The amount of biologically productive land and sea area needed to regenerate the resources a human population consumes.

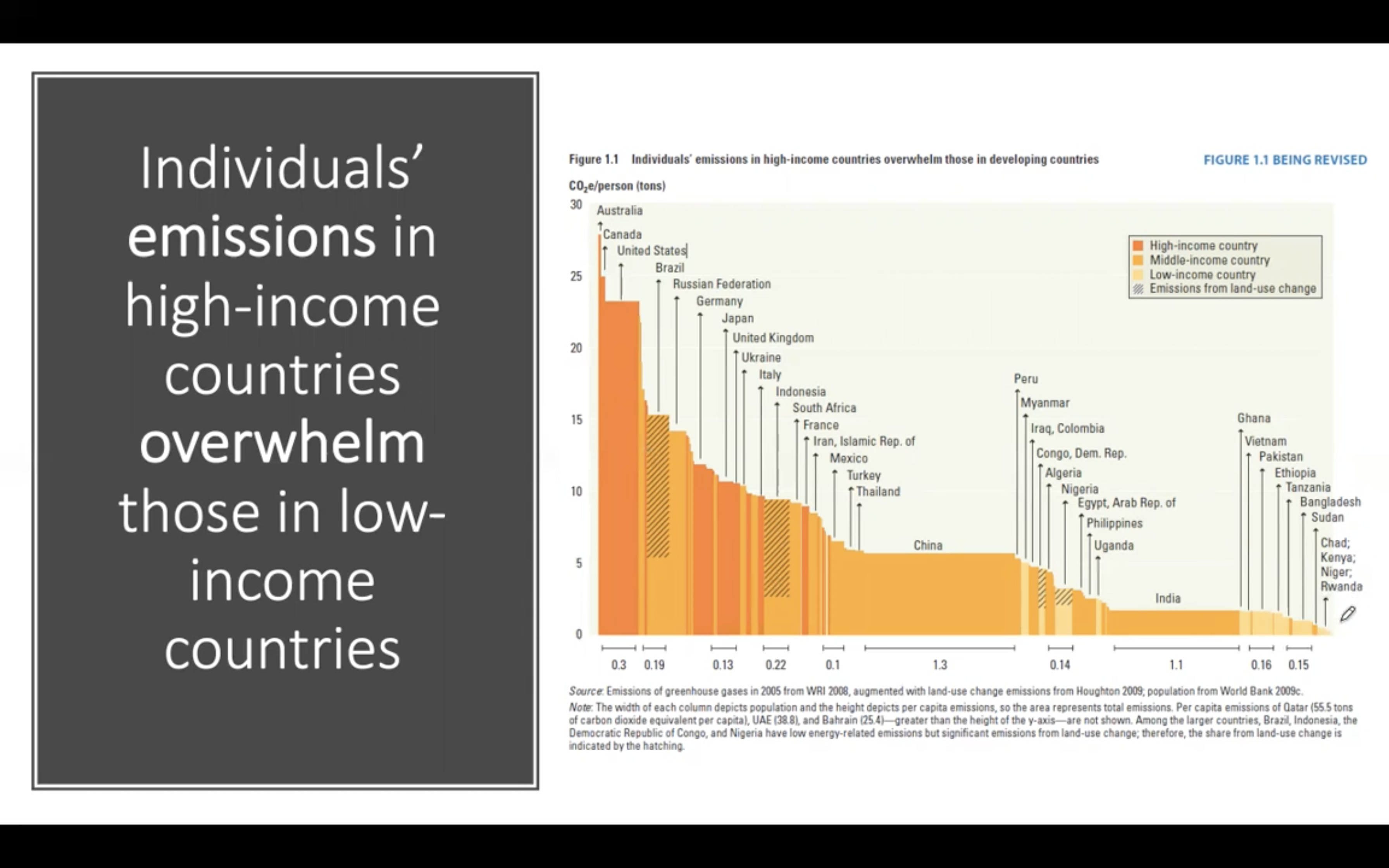
high income country emit more CO2
high income country emission per person (China vs Australia) overwhelm those in low income countries
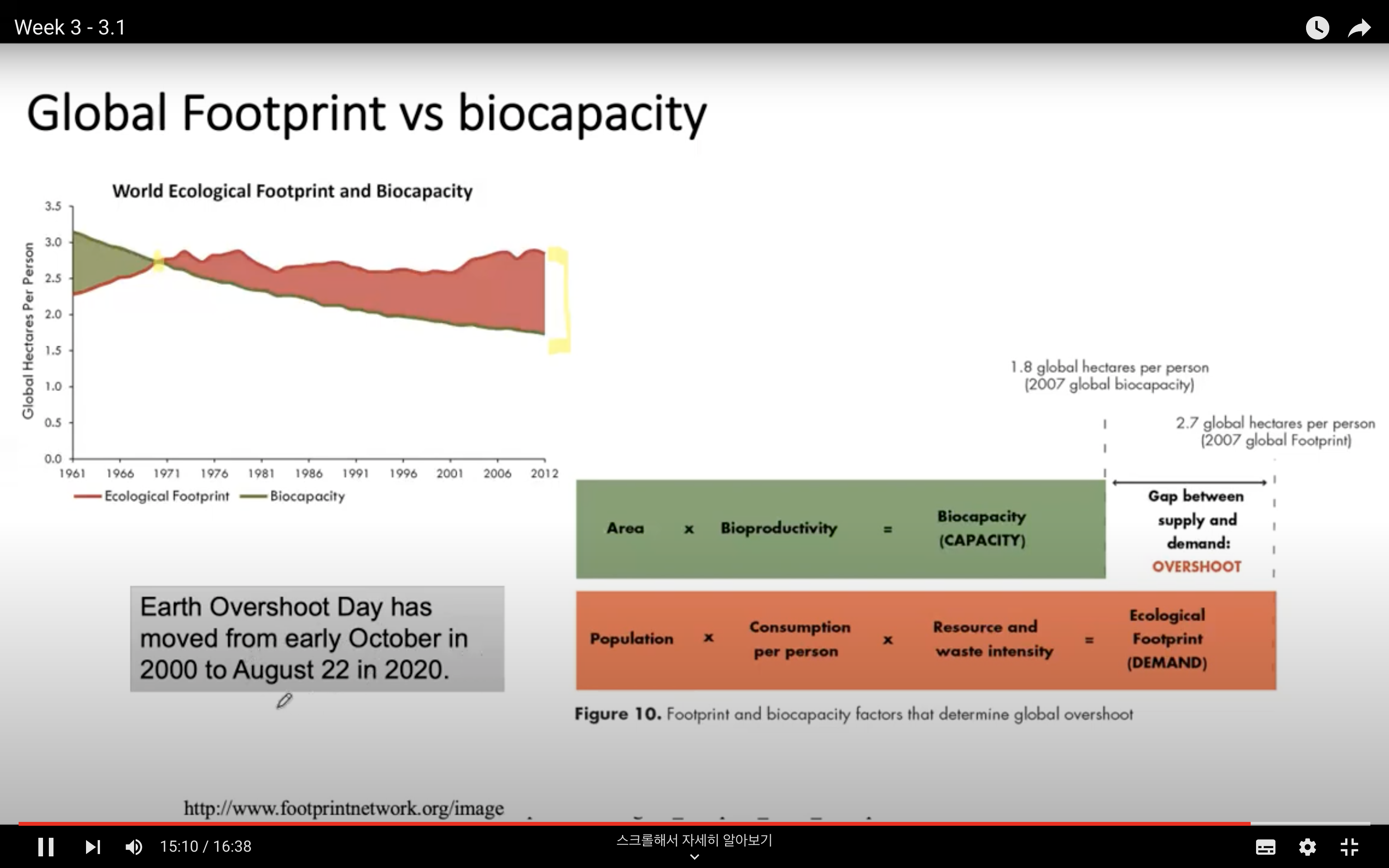
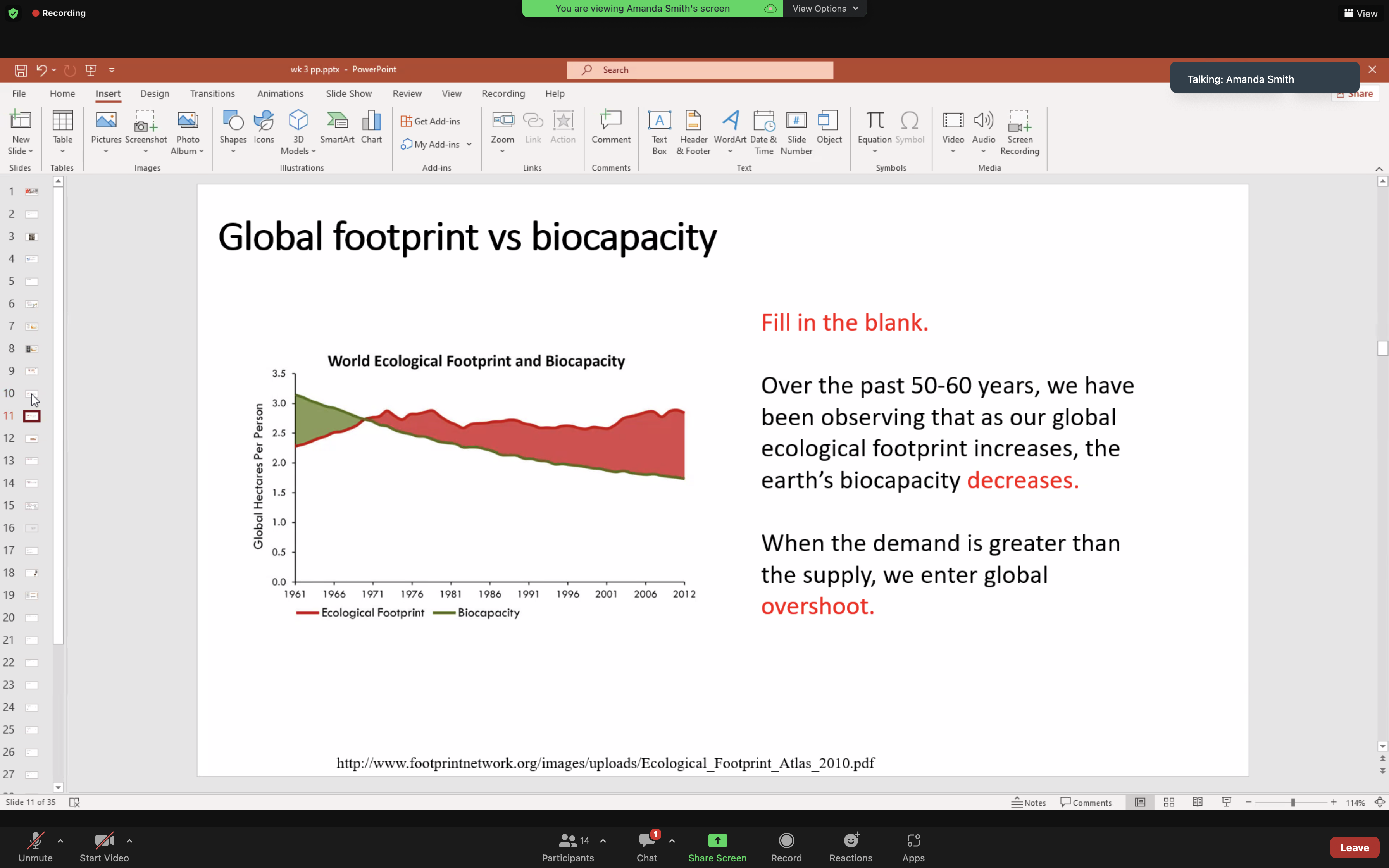
Global overshoot day
area x bioproductivity = biocapacity(capacity) SUPPLY
population x consumption per person x resource and waste intensity = ecological foot print DEMAND
ecological foot print - biocapacity = overshoot GAP between SUPPLY and DEMAND
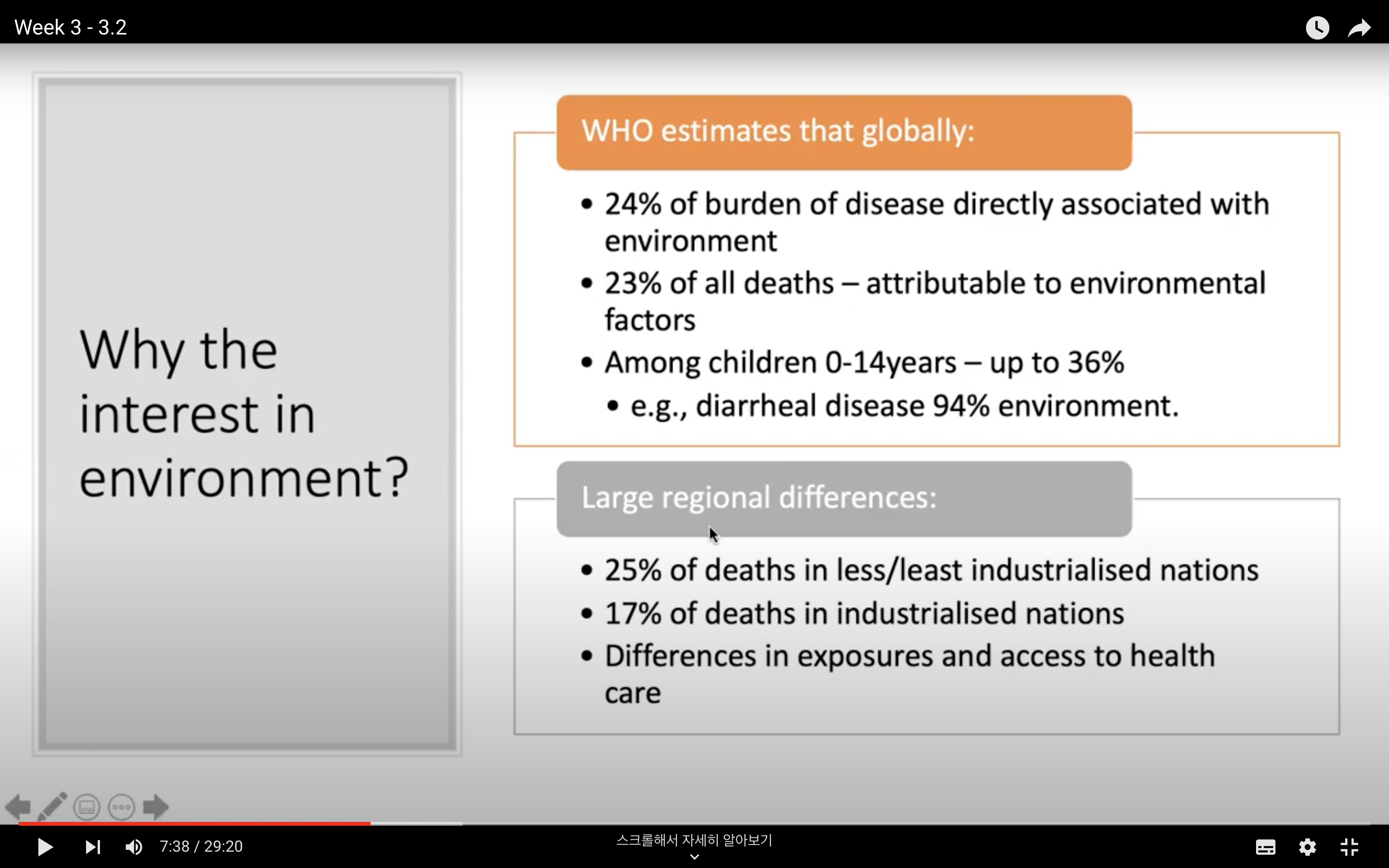
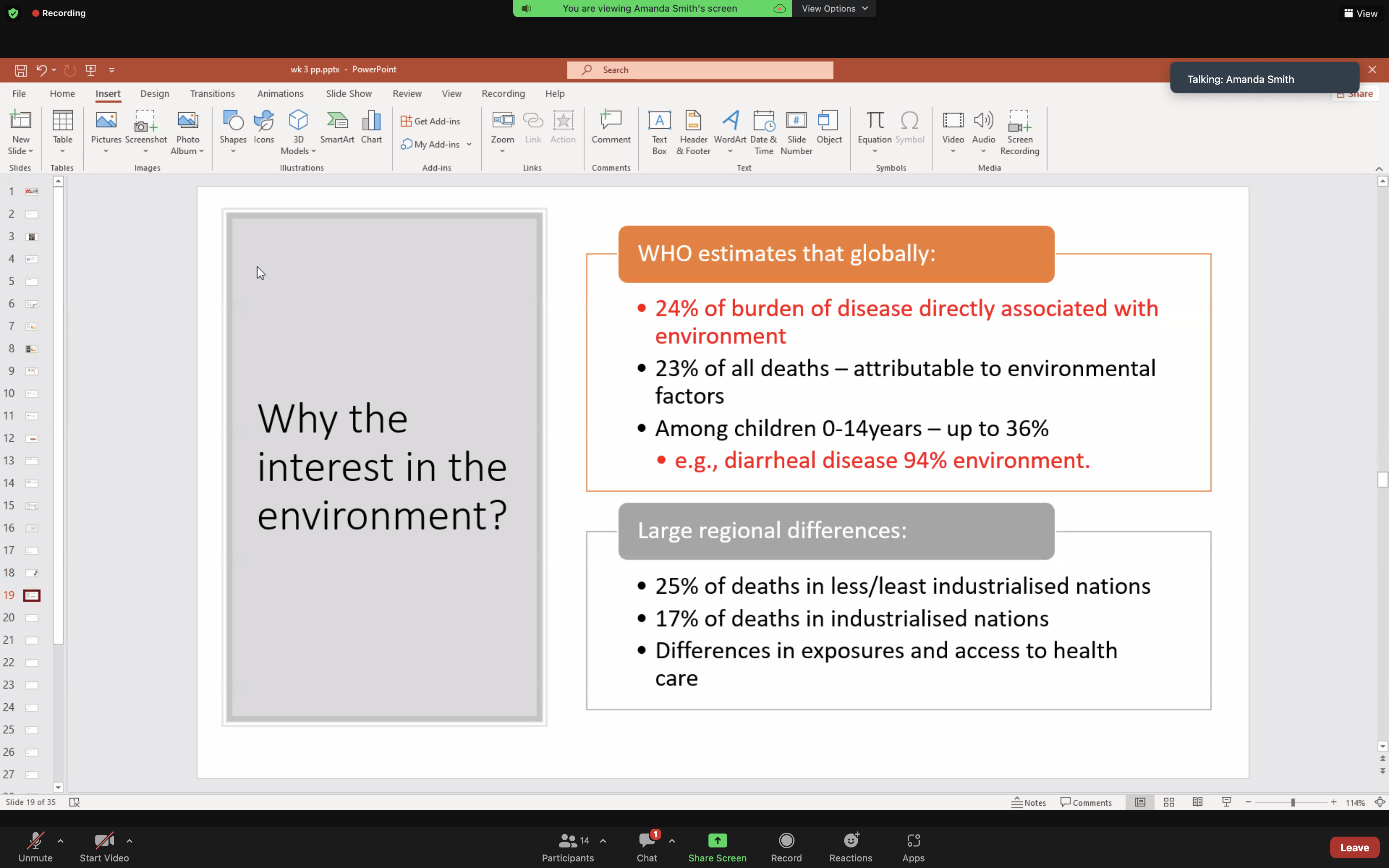
2. Burden of disease attributed to the environment
3.2 learning outcomes:
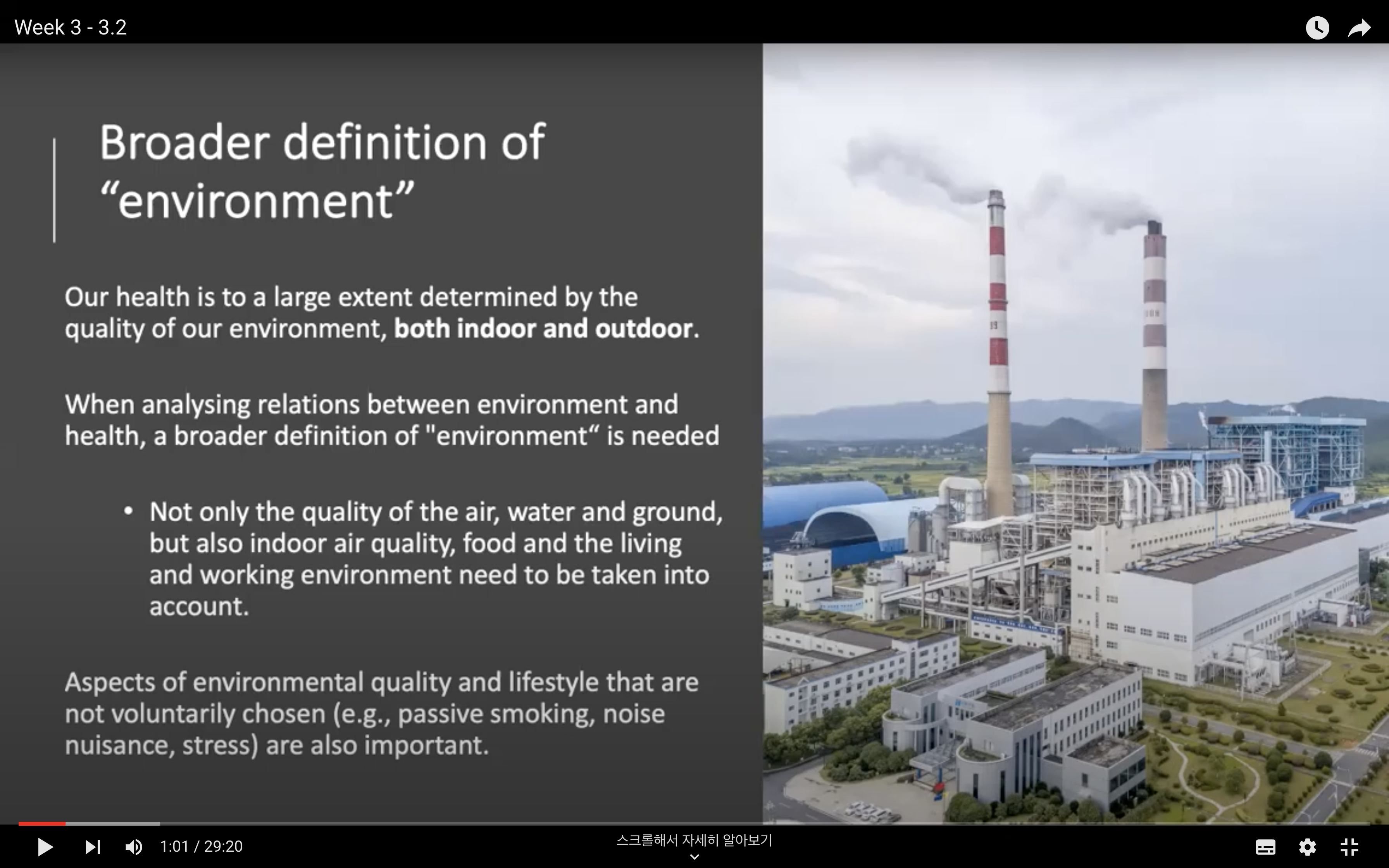
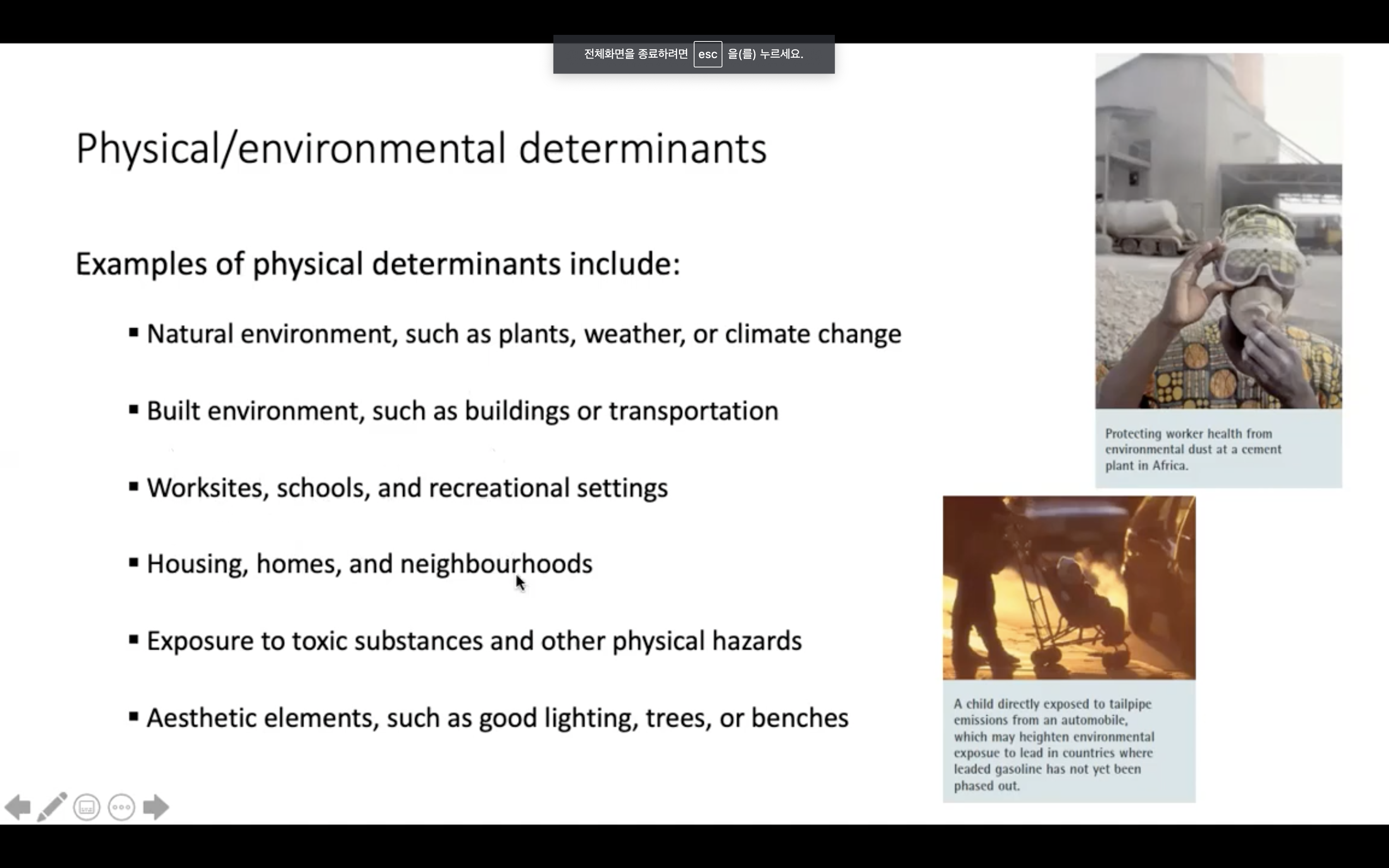
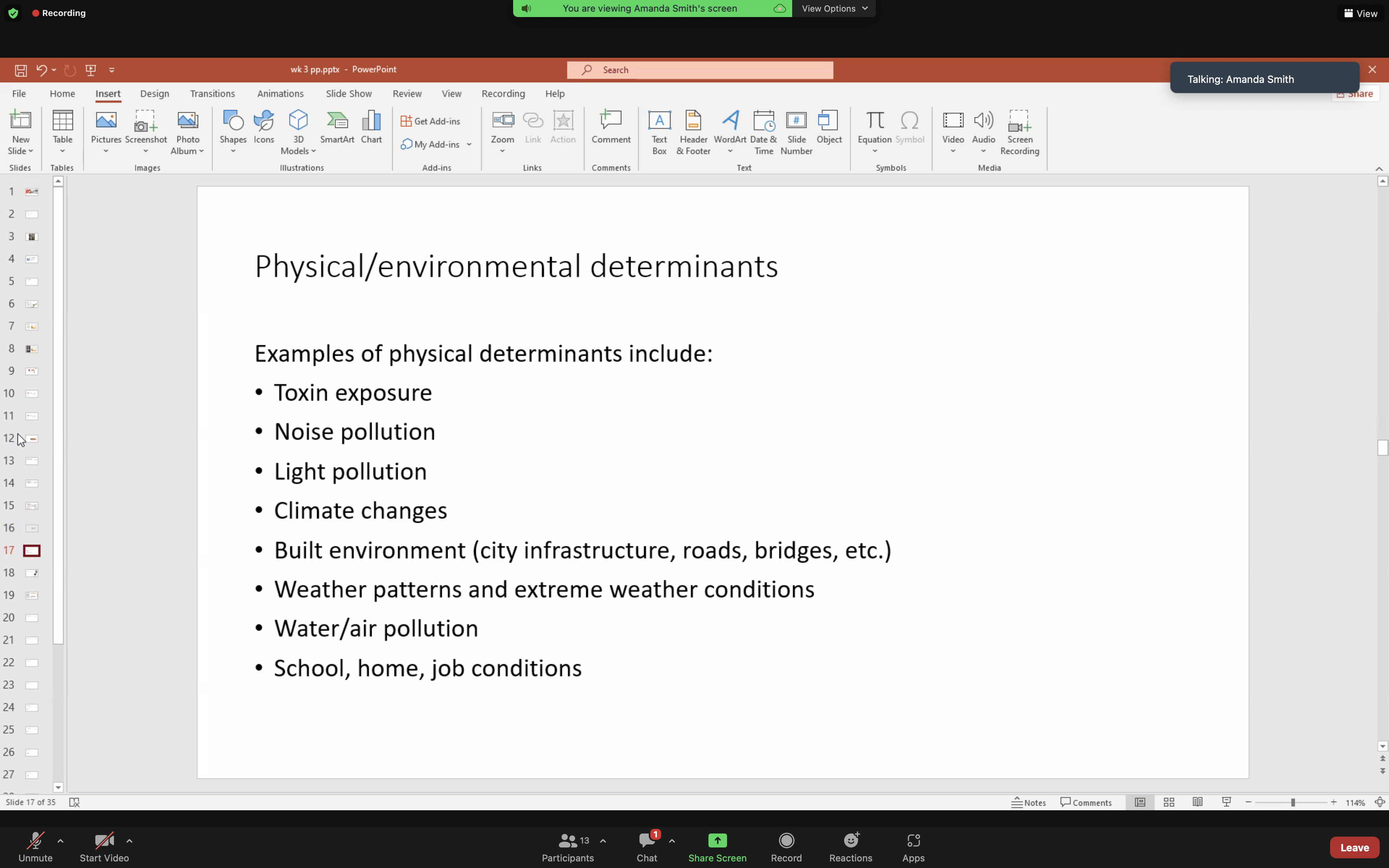
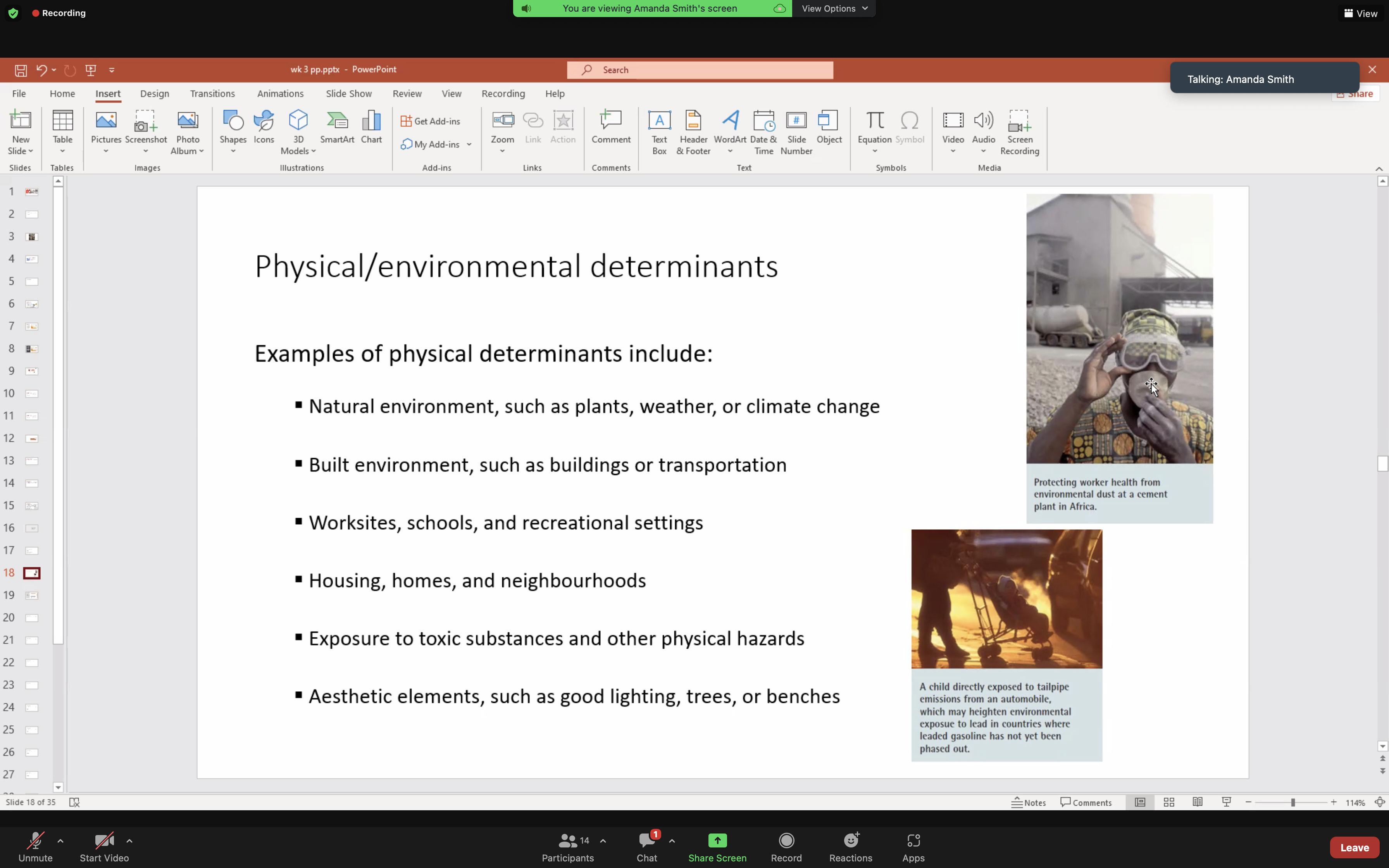
Physical environmental determinants
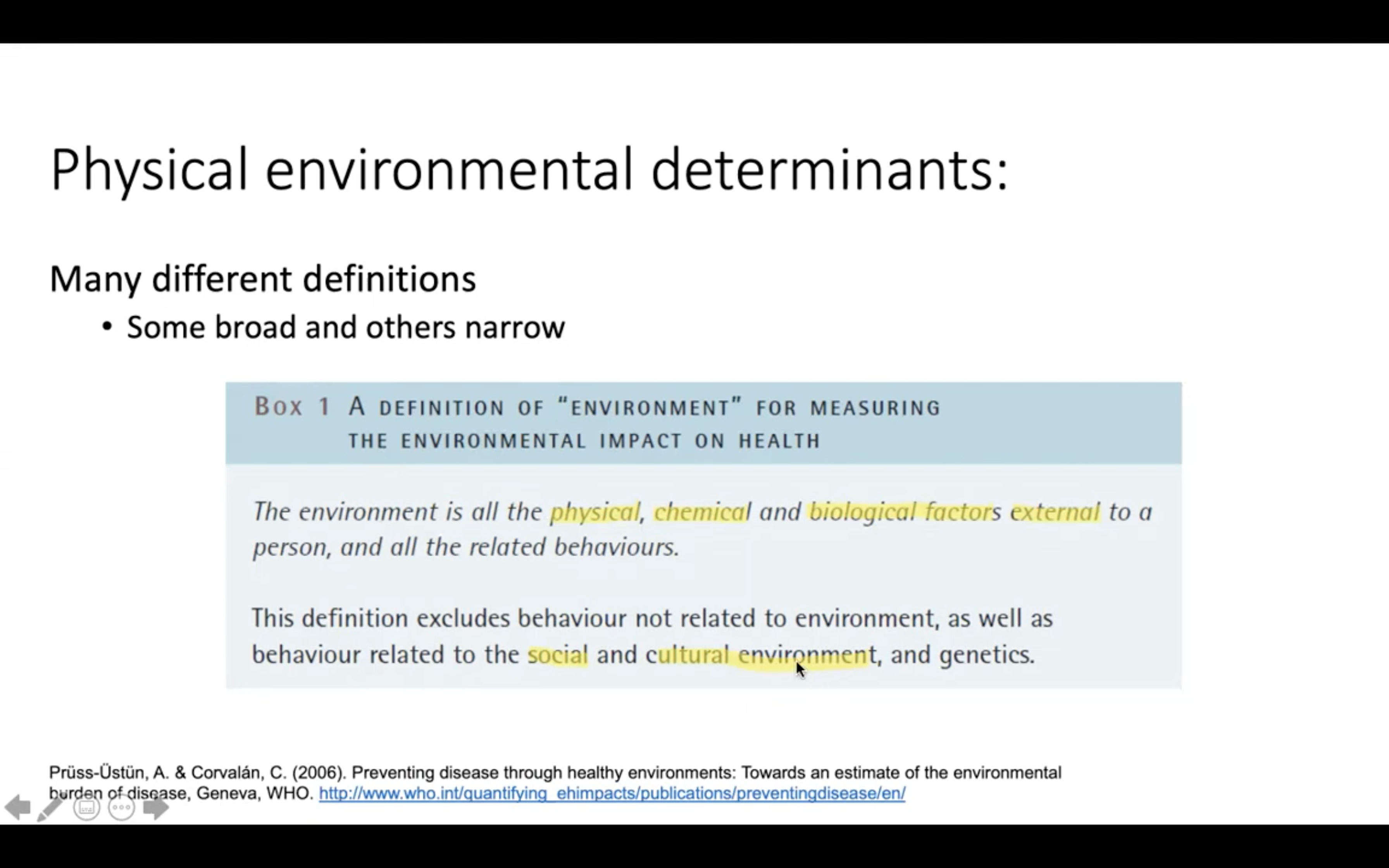
= A definition of "environment" for measuring the environmental impact on health.
-> The environment is all the physical, chemical and biological factors external to a person, and all the related behaviours. This definition excludes behaviour not related to environment, as well as behaviour related to the social and cultural environment, and genetics
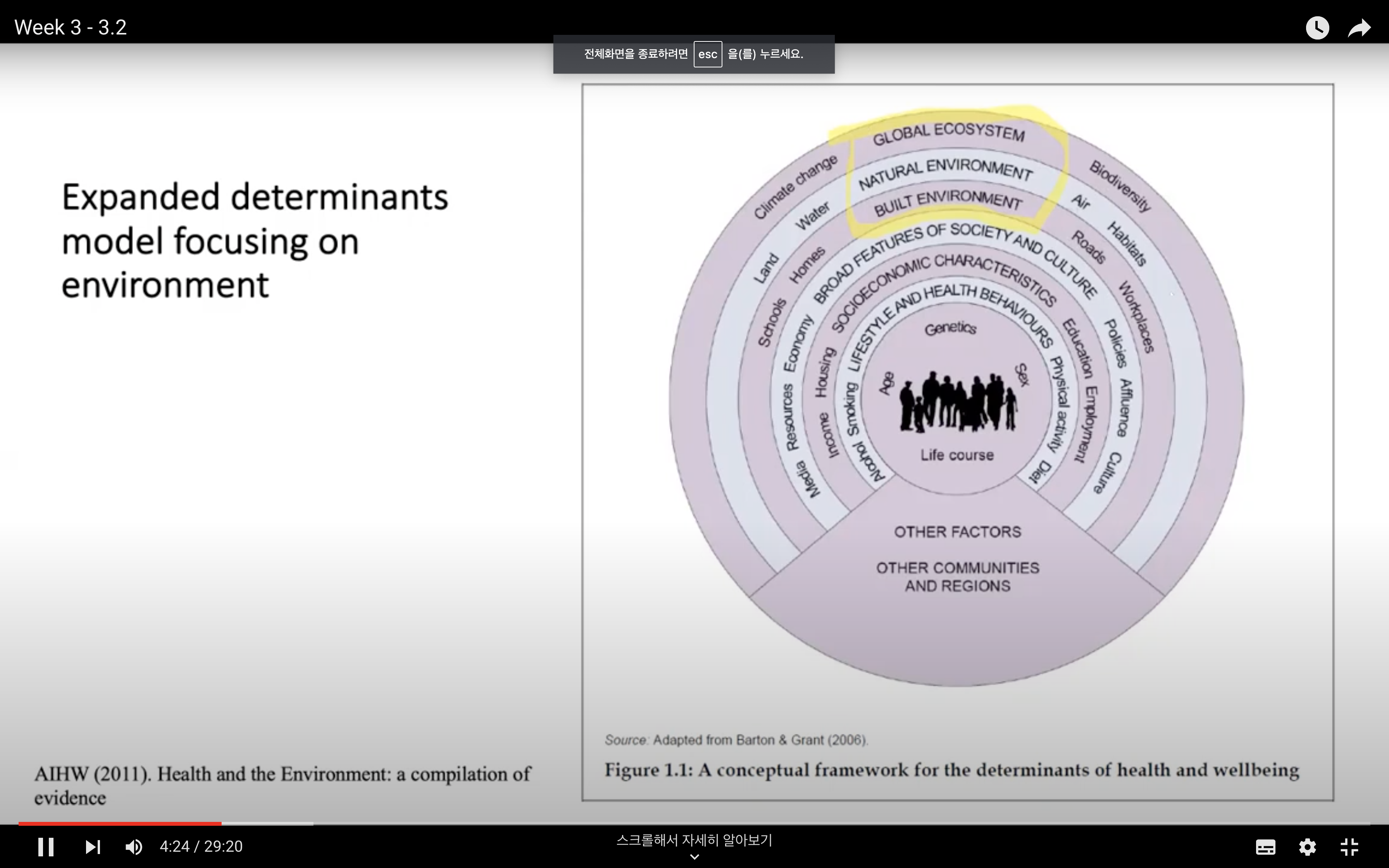
Expanded determinants model focusing on environment
: Built environment ( Schools, house, roads, workplaces) Natural environment (Land, Water, Air, Habitats), Global Ecosystem (Climate change, Biochemistry..)
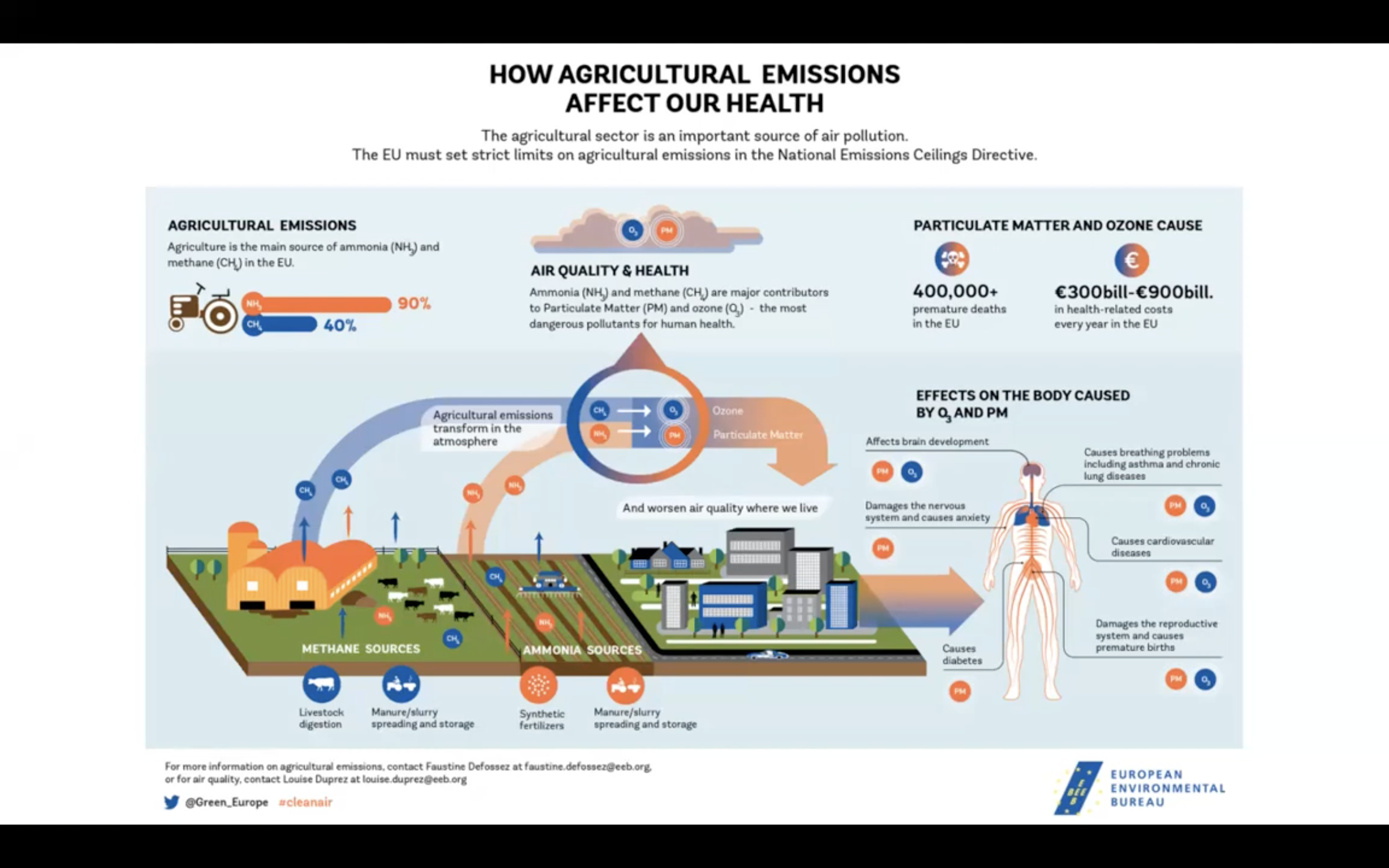
burning of cooking oils (cooking over hot oils) -> air pollution in indoor


- Define what is an environmental determinant
- Understand the link between several environmental determinants and human health
Questions to ask yourself:
A definition of "environment" for measuring the environmental impact on health.
After class
1. Required Resources
Please read the following excerpt from Chapter 7: Physical and Social Environmental Factors - Health in International Perspective: Shorter Lives, Poorer Health. doi: 10.17226/13497.
Physical Environmental Factors
The factors in the physical environment that are important to health include harmful substances, such as air pollution or proximity to toxic sites (the focus of classic environmental epidemiology); access to various health-related resources (e.g., healthy or unhealthy foods, recreational resources, medical care); and community design and the “built environment” (e.g., land use mix, street connectivity, transportation systems).
The environment can affect health through physical exposures, such as air pollution (OECD, 2012b). A large body of work has documented the effects of exposure to particulate matter (solid particles and liquid droplets found in the air) on cardiovascular and respiratory mortality and morbidity (Brook et al., 2010; Laumbach and Kipen, 2012; Mustafić et al., 2012; Tzivian, 2011). Research has identified specific physiologic mechanisms by which these exposures affect inflammatory, autonomic, and vascular processes (Brook et al., 2010; Tzivian, 2011).
The effects of particulate matter on mortality appear to be consistent across countries. For example, a recent review of studies from the late 1990s to mid-2000s found a consistent inverse relationship between airborne particulate matter and birth weight in Australia, Brazil, Canada, France, Italy, the Netherlands, South Korea, the United Kingdom, and the United States (Parker et al., 2011a). Another notable example is the evidence linking lead exposures to cognitive development in children (Bellinger, 2008; Levin et al., 2008). The evidence of environmental effects of air pollution and lead has been reflected in legislation in many countries directed at reducing levels of these pollutants in the environment.
Increasing attention has focused on the implications for health behaviors and social interactions that are created by the built environment. The built environment refers to the presence of (and proximity to) health-relevant resources as well as to aspects of the ways in which neighborhoods are designed and built (including land use patterns, transportation systems, and urban planning and design features). An important example is evidence that links proximity to healthy or unhealthy food stores with dietary behaviors and related chronic disease outcomes (Babey et al., 2008; Larson et al., 2009; Moore et al., 2008; Morland et al., 2006).4 Food availability and food advertising influence energy intake and the nutritional value of foods consumed (Grier and Kumanyika, 2008; Harris et al., 2009; Institute of Medicine, 2006a).
Another large body of work has documented how walking and physical activity levels are affected by access to recreational facilities, land use mix, transportation systems, and urban planning and design (Auchinloss et al., 2008; Diez Roux et al., 2001; Ding et al., 2011; Durand et al., 2011; Gordon-Larsen et al., 2006; Heath, 2009; Kaczynski and Henderson, 2008; McCormack and Shiell, 2011; Transportation Research Board, 2005). Studies conducted in the United States and other high-income countries have found that “walkability” (which is measured by such proxies as building density, land use mix, and street connectivity) predicts walking patterns (Durand et al., 2011; Inoue et al., 2009; Sundquist et al., 2011; Van Dyck et al., 2010). Across countries, studies have also shown that physical activity by children is associated with features of the built environment, including walking-related features, and physical activity resources (Bringolf-Isler et al., 2010; Davison and Lawson, 2006; Galvez et al., 2010; Sallis and Glanz, 2006).5
Although more definitive evidence is needed (see Feng et al., 2010), it has been hypothesized that these environmental features may contribute to the obesity epidemic (Galvez et al., 2010; Papas et al., 2007; Sallis and Glanz, 2009). The importance of residential environments to obesity and related conditions, such as diabetes, was recently highlighted by a randomized housing intervention: low-income participants who were randomly assigned to move into low-poverty areas experienced significant improvements in weight and diabetes indicators (Ludwig et al., 2011). Unfortunately, the study was not designed to identify the specific environmental features responsible for the observed effect.
A range of other physical environmental features have been linked to other health outcomes. For example, the density of alcohol retail outlets has been linked to alcohol-related health complications (Campbell et al., 2009; Popova et al., 2009), including injury and violence (Cunradi et al., 2012; Toomey et al., 2012). Transportation systems and other aspects of physical environments that influence driving behaviors are also related to injury morbidity and mortality (Douglas et al., 2011). Living in socioeconomically disadvantaged neighborhoods (as a proxy for a range of environmental exposures) has been linked to higher rates of injury in both adults and children (Cubbin et al., 2000; Durkin et al., 1994).
Social Environmental Factors
Factors in the social environment that are important to health include those related to safety, violence, and social disorder in general, and more specific factors related to the type, quality, and stability of social connections, including social participation, social cohesion, social capital, and the collective efficacy of the neighborhood (or work) environment (Ahern and Galea, 2011).6 Social participation and integration in the immediate social environment (e.g., school, work, neighborhood) appear to be important to both mental and physical health (DeSilva et al., 2005). What also seems important is the stability of social connections, such as the composition and stability of households7 and the existence of stable and supportive local social environments or neighborhoods in which to live and work.
A network of social relationships is an important source of support and appears to be an important influence on health behaviors. Work on the “transmission” of obesity through social networks has highlighted the possible importance of social norms in shaping many health-related behaviors (Christakis and Fowler, 2007; Hruschka et al., 2011; Kawachi and Berkman, 2000).8 A long tradition of sociological research links these social features not only to illness, but also to risks of violence (Morenoff et al., 2001; Sampson et al., 1997). Social environments may also operate through effects on drug use, which also has consequences for violence and mental-health-related outcomes.9
Neighborhood conditions can create stress (Cutrona et al., 2006; Do et al., 2011; Merkin et al., 2009), which have biological consequences (see Chapter 6). Features of social environments that may operate as stressors (including perceptions of safety and social disorder) have been linked to mental health, as have factors that could buffer the adverse effects of stress (e.g., social cohesion, social capital) (DeSilva et al., 2005; Mair et al., 2008).
One mechanism through which the social environment can enhance health is through social support. Social support has appeared in many (but not all) studies to buffer the effects of stress (Cohen and Wills, 1985; Matthews and Gallo, 2011; Ozbay et al., 2007, 2008). Resilience to the adverse health effects of stress has also been tied to factors that could influence how one perceives a situation (threat versus challenge) and how one responds to stressors (Harrell et al., 2011; Hennessy et al., 2009; Matthews and Gallo, 2011; Ziersch et al., 2011). One theory for the tendency of some immigrant groups to have better health outcomes than might be expected on the basis of their incomes and education (see Chapter 6) is the social support immigrants often provide one another (Matthews et al., 2010).
Social capital refers to “features of social organization, such as trust, norms, and networks, that can improve the efficiency of society by facilitating coordinated actions” (Putnam, 1993, p. 167). Studies have shown consistent relationships between social capital and self-reported health status, as well as to some measures of mortality (Barefoot et al., 1998; Blakeley et al., 2001; Kawachi, 1999; Kawachi et al., 1997; OECD, 2010c; Schultz et al., 2008; Subramanian et al., 2002). Social capital depends on the ability of people to form and maintain relationships and networks with their neighbors. Characteristics of communities that foster distrust among neighbors, such as neglected properties and criminal activity, can affect both the cohesiveness of neighbors as well as the frequency of poor health outcomes (Center on Human Needs, 2012b).
Spatial Distribution of Environmental Factors
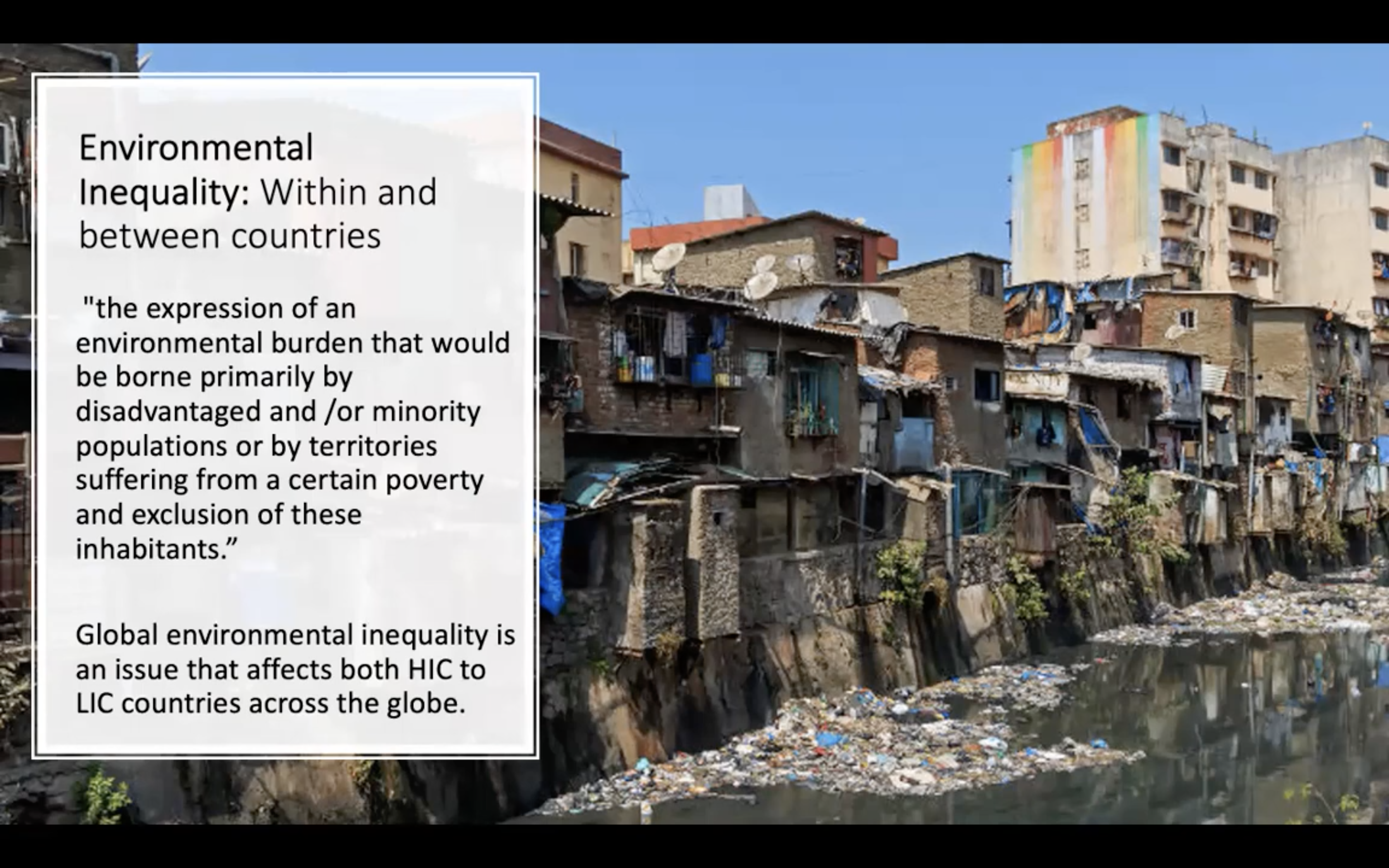
In addition to considering differences between the United States and other countries in the absolute levels of environmental factors, it is also important to consider how these factors are distributed within countries. Levels of residential segregation shape environmental differences across neighborhoods (Reardon and Bischoff, 2011; Subramanian et al., 2005).
Neighborhoods with residents who are mostly low-income or minorities may be less able to advocate for resources and services. Perceptions and stereotypes about area reputation, local demand for products and services, and the purchasing power of residents may also influence the location of health-relevant resources. Physical environmental threats (such as proximity to hazardous sites) may be more prevalent in low-income or minority neighborhoods, a concern of the environmental justice movement (Brulle and Pellow, 2006; Evans and Kantrowitz, 2002; Mohai et al., 2009; Morello-Frosch et al., 2011). These neighborhoods may also lack the social connections and political power that can help remedy adverse conditions.
Other Environmental Considerations
The panel focused its attention on the role of local physical and social environments as potential contributors to the U.S. health disadvantage and did not systematically examine whether other contexts, such as school or work environments, differ substantially across high-income countries. Nor did the panel examine whether neighborhood conditions exert a greater influence on access to health care in the United States than in peer countries. However, these conditions are important to health. For example, the school environments of children, adolescents, and college students can affect diet, physical activity, and the use of alcohol, tobacco, and other drugs (Katz, 2009; Wechsler and Nelson, 2008). Dietary options on cafeteria menus and in vending machines, opportunities for physical activity, and health education curricula are all important to children’s health.
Workplaces have also long been recognized as important determinants of health and health inequalities, occupational safety, and access to preventive services (Anderson et al., 2009; Schulte et al., 2011). Physical working conditions (e.g., exposure to dangerous substances, such as lead, asbestos, mercury), as well as physical demands (e.g., carrying heavy loads), human factors, and ergonomic problems can affect the health and safety of employees. Stressful psychosocial work environments and “job strain”—which refers to high external demands on a worker with low levels of control or rewards—have become recognized as prominent determinants of health and have been linked to self-reported ill health (Stansfeld et al., 1998), adverse mental health outcomes (Clougherty et al., 2010; Low et al., 2010; Stansfeld and Candy, 2006), and markers of chronic disease (Fujishiro et al., 2011). Exposure to job strain exhibits a strong social gradient, which influences inequalities in the health of workers (Bambra, 2011).10
(Optional) want to read more? The full book can be accessed here: https://www.nap.edu/read/13497/chapter/1
'Griffith college Tri3 2022 > 1205MED (Health challenges)' 카테고리의 다른 글
| WEEK5 (0) | 2022.11.30 |
|---|---|
| WEEK4 (0) | 2022.11.13 |
| WEEK2 - Essay 과제 설명 (0) | 2022.11.02 |
| WEEK2 (0) | 2022.11.02 |
| WEEK1 (0) | 2022.10.26 |



